Seating As We Age August 1, 2014 by Laurie Watanabe another opinion A “Radical Departure” http://cirrie.buffalo.edu/encyclopedia/en/article/288/
Briefly: NCART Joins YouTube; ALS Treatment Withdrawn After Trial Results Featuring the National Coalition for Assistive & Rehab Technology and Amylyx Pharmaceuticals.
Cure SMA Annual Community Update Survey Now Open The organization is seeking input from adults with spinal muscular atrophy.
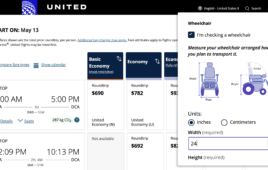
Numotion, United Spinal Collaborate with United Airlines on Wheelchair Fit Tool Wheelchair riders can check a flight’s ability to accommodate their mobility devices.
, 1-14.</p>
<p>Campbell ML, Sheets DS, Strong PS. 1999. Secondary health conditions among middle-aged individuals with chronic physical disabilities: Implications for “unmet needs” for services. Assistive Technology 11(2):3-18.</p>
<p>Sheets D. 2010. Aging with Physical Disability. In: JH Stone, M Blouin, editors. International Encyclopedia of Rehabilitation. Available online: <a href=) http://cirrie.buffalo.edu/encyclopedia/en/article/288/http://cirrie.buffalo.edu/encyclopedia/en/article/288/
http://cirrie.buffalo.edu/encyclopedia/en/article/288/http://cirrie.buffalo.edu/encyclopedia/en/article/288/